Cricothyrotomy Simulator
Safety & Quality
Safety & Quality
👉 This product is for training purposes only.
❓ It is unknown if this product contains Latex.
✅ Sim & Skills is ISO 9001 certified.
✅ Available via NHS Supply Chain.
Delivery
Delivery
When will my order arrive?
Items listed as In Stock are usually delivered in 1-3 working days.
Due to global supply chain disruption, some products are taking longer to deliver. If your order is affected, we will inform you as soon as possible with an estimated lead time or an alternative product recommendation.
For urgent or high volume orders, please contact us before placing your order to check stock availability.
How much does delivery cost?
Tracked Delivery on website orders to a single Mainland Great Britain address is charged at £7.50 + VAT.
Tracked Delivery on purchase orders to a single Mainland Great Britain address is charged at £15.00 + VAT.
Shipping to Northern Ireland and British Forces is charged at £25.00 + VAT.
Palletised deliveries are charged at £85.00 + VAT per pallet.
Deliveries will be made to a Goods In area not a specific room/department.
International shipping is provided on a case-by-case basis, please contact us for a quote.
Returns
Returns
What is the returns policy?
Returns are acceptable within 28 days of delivery (by law you have 14 days to notify us and a further 14 days to complete the return), providing the item is in a resalable condition and in its undamaged original packaging.
Cancellations and Returns are free of charge for items up to 20 kg. Collection for items over 20 kg will be quoted on a case-by-case basis.
All returns must be pre-authorised prior to shipping. Unauthorised returns may be refused and additional carriage costs may be incurred.
Failure to return goods in a resalable condition may result in a restocking fee of £25.00 + VAT or 20% of the invoice value, whichever is greater.
Any goods returned for product defect or warranty issues will not incur a restocking fee, but must still have appropriate authorisation.
To start a return, email orders@simandskills.com.
If your return is accepted, we’ll send you a return shipping label and instructions on how and where to send your package. Items sent back to us without first requesting a return will not be accepted.

Cricothyrotomy Simulator
Description
Description
Cricothyrotomy Simulator
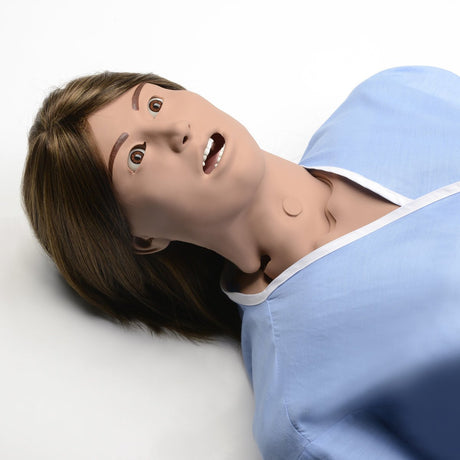
The newly designed Lifeform Cricothyrotomy Simulator has been developed for learning and practising the techniques necessary to perform needle or surgical cricothyrotomy procedures.
Paramedics, EMTs, combat medics, flight nurses, anaesthesiologists and other emergency medical personnel will have the opportunity to strengthen their ability and confidence to perform or assist in implementing surgical airways. Anatomically accurate landmarks aid in site training and allow for fast action.
The hyperextended neck allows the user to determine the proper incision site. The trachea in the simulator is replaceable, as the airway passes completely through from top to bottom. This allows checking the stylet and obturator placement once the incision has been made.
Complete with a chin and full-size neck, use ties to hold the obturator in a secure position. Inflation of the simulated lung verifies correct placement.
About Cricothyrotomy
A cricothyrotomy is often used as an airway of last resort given the numerous other airway options available including standard tracheal intubation and rapid sequence induction, which are the common means of establishing an airway in an emergency scenario.
Cricothyrotomies account for approximately 1% of all emergency department intubations and are used mostly in patients who have experienced a traumatic injury.
Indications for Cricothyrotomy
Some general indications for this procedure include:
-
Inability to intubate
-
Inability to ventilate
-
Inability to maintain SpO2 >90%
-
Severe traumatic injury that prevents oral or nasal tracheal intubation
Contraindications
-
Inability to identify landmarks (cricothyroid membrane)
-
Underlying anatomical abnormalities such as a tumour or severe goitre
-
Tracheal transection
-
Acute laryngeal disease due to infection or trauma
-
Small children under 12 years old (a 10–14 gauge catheter over the needle may be used)
Procedure
The procedure was first described in 1805 by Félix Vicq-d'Azyr, a French surgeon and anatomist. A cricothyrotomy is generally performed by making a vertical incision on the skin of the throat just below the laryngeal prominence (Adam's apple), then making another transverse incision in the cricothyroid membrane which lies deep to this point.
A tracheostomy tube or endotracheal tube with a 6 or 7 mm internal diameter is then inserted, the cuff is inflated, and the tube is secured. The person performing the procedure might utilise a bougie device, a semi-rigid, straight piece of plastic with a one-inch tip at a 30-degree angle, to provide rigidity to the tube and assist with guiding its placement.
Confirmation of placement is assessed by bilateral auscultation of the lungs and observation of the rise and fall of the chest. Alternatively, bedside ultrasound has been used increasingly to guide the procedure and confirm the placement of the tracheal tube. It may especially be helpful in situations where a neck collar is placed.
Training
This procedure is rarely performed, given advancements in airway technique and adjuncts, and thus simulated training is of paramount importance to correctly perform this procedure under a high-stress situation.
Specifications
Specifications
-
Manufacturer's Warranty5 Years
Reviews (0)
Reviews (0)
Payment & Security
Secure payment methods
Your payment information is processed securely. We do not store or have access to your credit card details.
Purchase Orders
We accept purchase orders from public and government authorities including the NHS and Universities subject to our terms of business.
Click Add to Quote to easily build your quote ➡️
Let customers speak for us

Very life like ,easy to use

The quality is amazing 🥰
Amazing
But recommend the sutures to be 2/0.
4/0 is very small
I'm a medical student and was really pleased with the quality of this kit, all the tools are well made and the case is near and sturdy

Works well
If i could give it 4.5 I would but I'm much more inclined to say I'm happy with this product. Really good quality, excellent resource for my vet suturing practice. I have a mild complaint about the silk sutures, they rip/ fray more easily than I hoped, but easily rectified by buying new ones (which are cheap) and also encourages me to be more gentle with my knots. I'm so happy with it and it's a perfect still revising break from studying. Thank you Sim and Skills!!!

Student Feedback: Feedback was gathered from 13 students. Overall, they liked the trainer and would recommend it to their peers for learning blood glucose testing. They found the trainer easy to use and helpful in demonstrating the procedure. The students felt that the trainer added significant value to their training, with the main benefit being an increased competency in blood glucose testing.
Lecturer Feedback: Feedback was collected from 7 lecturers. Most of them found the trainer to be authentic and effective in simulating the challenges of blood sugar testing. They appreciated that it encouraged patient communication, which is a great plus. The product was of good quality and reliable for teaching purposes. However, there was a minor issue with the finger becoming leaky after multiple uses. Despite this, the lecturers agreed that the trainer prepares students well for real-world blood glucose testing.

Excellent service and speedy delivery. Highly recommended
Brilliant teaching aid. Lots of useful equipment within set. Excellent for practice.
Amazing product

As a proud owner of a Sim & Skills Foot & Ankle model, I thought it was time I invested in a Hand & Wrist.
My clients find it really helpful when we are discussing anatomy and it really aids their recovery.
I believe client education and knowing that your body is something to be enjoyed, not feared, is such an important platform for recovery from chronic pain.

This item is very useful for NG insertion training, it can be used in a horizontal position and the fluid bag does not leak out. The bag and tubing can all be stored within the head making storage of the item easy. It is very simple to use and the head is strong and durable
Purchased these bags for training with venepuncture and so far very pleased with quality and cost

Fast delivery, excellent communication and a great price

Excellent fast service. Thank you.